COPD (Chronic Obstructive
COPD (Chronic Obstructive Pulmonary Disease): Overview
Alternative names: Known to many as chronic bronchitis or emphysema.
Chronic Obstructive Pulmonary Disease (COPD) refers to a group of conditions that cause shortness of breath and are associated with obstruction of air flow within the lung. Patients typically have symptoms of both chronic bronchitis and emphysema, but the classic triad also includes asthma.
Diagnose your symptoms now!
- check your overall health status
- let The Analyst™ find what's wrong
- learn what you should be doing right now
COPD is a combination of 3 separate disease processes that together form the complete clinical picture. These processes are chronic bronchitis, emphysema and, to a lesser extent, asthma. While each case of COPD is unique in the blend of processes, two main types of the disease are recognized.
Chronic Bronchitis – "Blue Bloaters"
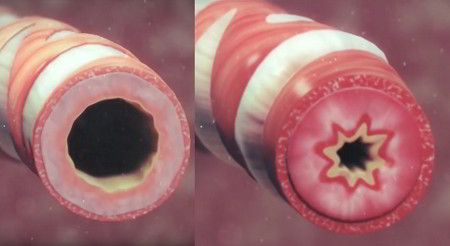
A healthy airway (left) and an airway damaged by Chronic Bronchitis (right). The lining swells, thickens, and produces mucus.
Chronic bronchitis plays the major role in this type of COPD and is defined by excessive mucus production with airway obstruction and notable enlargement of mucus-producing glands.
Damage to the airway lining impairs the miniature ciliary hairs located there which usually help clear bacteria and mucus. Inflammation and secretions provide the obstructive component of chronic bronchitis. In contrast to emphysema, chronic bronchitis is associated with a relatively undamaged pulmonary capillary bed. Emphysema is usually present to a variable degree.
As the disease progresses, these patients develop signs of right-sided heart failure and are known as "blue bloaters".
Emphysema – "Pink Puffers"
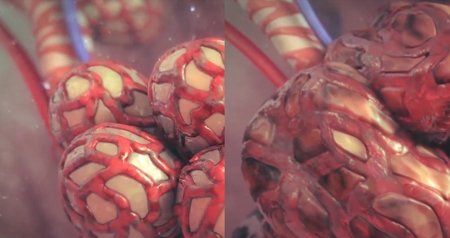
Normal alveoli (left), and damaged by Emphysema (right). Sacs combine into larger sacs and become harder to expand and contract.
The second major type of COPD is that in which emphysema is the primary underlying process. The physiology of emphysema involves the gradual destruction of the small air sacs (alveoli) where gas diffusion takes place, and of the pulmonary capillary bed, leading to a decreased ability to oxygenate blood. The body compensates with lowered cardiac output and more rapid breathing. Eventually, these patients develop muscle wasting and weight loss and are identified as "pink puffers".
Incidence; Causes and Development; Contributing Risk Factors
COPD is estimated to affect around 10% of the population in the United States, where it is also the fourth leading cause of death. COPD prevalence has increased dramatically in the past few decades and is one of the major causes of bed-confining disability. Men are more likely to have COPD than women, and it occurs mainly in those over 40.
Most of the time COPD is secondary to tobacco abuse, but other more rare conditions, such a cystic fibrosis, may be contributing factors.
Being obese can aggravate COPD.
Treatment and Prevention

Lung damage from COPD cannot be reversed: Alveoli have combined to form larger air sacs
There is no cure for Chronic Obstructive Pulmonary Disease, and the damage that has been done cannot be undone. However, through a combination of lifestyle changes and treatments, progress of the disease can be slowed and symptoms reduced.
Quitting smoking and avoiding other lung irritants (such as second-hand tobacco smoke, dust, fumes), are the most important first steps to take.
Those with COPD often have trouble eating and taking in sufficient nutrients, so smaller, more frequent nutrient-rich meals as well as supplements can be helpful.

Oxygen therapy for COPD using a nasal cannula
Oxygen therapy can help get more oxygen into the blood. Oxygen is delivered via an oxygen mask or a nasal cannula connected to an oxygen tank. Patients with severe COPD may require extra oxygen all the time in order to be able to function more normally. Having sufficient oxygen also protects the heart and other organs from damage, allows better sleep, improves alertness, and extends the patient's life.
As well as rehabilitation and exercise to improve overall well-being, medications are available to relieve symptoms:
- Bronchodilators (normally used in combination with steroids to reduce inflammation) open the airways and make breathing easier
- Flu shots reduce the risk of catching a flu, which can be very hard on those with COPD
- The Pneumococcal vaccine reduces the risk of getting pneumococcal pneumonia, which is more likely in those with COPD
Lung Volume Reduction Surgery (LVRS) removes some of the most diseased parts of the lungs
Surgery is the last resort in cases where other treatments are not alleviating symptoms. Three types of surgery are possible:
- A bullectomy, in which bullae (very large air sacs formed from hundreds of damaged alveoli) are removed
- Lung volume reduction surgery (LVRS), in which approximately the most damaged 30% of the lungs is removed in order to allow the remaining lung tissue to perform better
- Lung transplant in severe cases
Complications
Patients with COPD are susceptible to many factors that can lead to an acute deterioration. Aggressive and prompt intervention may be the only action that prevents respiratory failure.
On This Page
Chronic Bronchitis:Signs, symptoms & indicators of COPD (Chronic Obstructive Pulmonary Disease):
Symptoms - General
Symptoms - Nails
Symptoms - Respiratory
 difficult exhalation is often a sign or symptom of COPD (Chronic Obstructive Pulmonary Disease)") (Intermittent) difficult exhalation
(Intermittent) difficult exhalation
COPD causes the lungs to undergo permanent changes that affect one's ability to exhale properly. These changes usually worsen over time.
Counter-indicators
") Absence of difficult exhalation
Absence of difficult exhalation
COPD causes the lungs to undergo permanent changes that affect one's ability to exhale properly. These changes usually worsen over time.
Conditions that suggest COPD (Chronic Obstructive Pulmonary Disease):
Circulation
Respiratory
") Pneumonia
Pneumonia
Lung diseases – such as chronic bronchitis and emphysema – are risk factors for the development of pneumonia.
Symptoms - Respiratory
Counter-indicators
Risk factors for COPD (Chronic Obstructive Pulmonary Disease):
Lab Values - Scans
Counter-indicators
Symptoms - Muscular
Being lean or underweight or being very skinny
Slender, older women are more susceptible to various chronic lung problems such as bronchitis, pneumonia and asthma, according to a long series of studies.
Concerned or curious about your health? Try The Analyst™

Symptom Entry

Diagnosis

Suggestions

LifeMeter®

Explanations

Review (optional)
COPD (Chronic Obstructive Pulmonary Disease) suggests the following may be present:
Addictions
Cigarette Smoke Damage
Smoking is the single most important risk factor in the development of COPD, contributing to 81.5% of all COPD deaths. People who smoke or have chronic bronchitis have an increased risk of emphysema. Chronic coughing and shortness of breath are symptoms of these diseases. Studies involving over one million men and women have shown that the death rate for chronic bronchitis and emphysema is six times as high for smokers as for non-smokers.
Diet
Consequences of Poor Diet
Out of 50 consecutive COPD patients presented with acute respiratory failure upon admittance to a hospital, malnutrition was observed in 60% of all patients but only 39% of those whose body weight was equal to or above 90% of ideal body weight. These results suggest that assessment of nutritional status should be systemically performed for COPD patients with acute respiratory failure, especially those who are in need of mechanical ventilation. Aggressive, early nutritional support in acute illness might have beneficial effects on the weaning of patients off mechanical intervention. [Nutritional Status of Patients With COPD and Acute Respiratory Failure, Chest, May 1993;103(5): pp.1362-68]
Recommendations for COPD (Chronic Obstructive Pulmonary Disease):
Amino Acid / Protein
 may help with COPD (Chronic Obstructive Pulmonary Disease)") Cysteine / N-Acetylcysteine (NAC)
Cysteine / N-Acetylcysteine (NAC)
NAC helps break down mucus. Double-blind research has found that NAC supplements improved symptoms and prevented recurrences in people with chronic bronchitis. NAC may also protect lung tissue through its antioxidant activity.
Botanical / Herbal
Diet
") High/Increased Protein Diet
High/Increased Protein Diet
Researchers from England state that chronic obstructive pulmonary disease may only worsen by eating a diet that contains an overabundance of high-carbohydrate foods. The results suggest that even small changes in the constitution of meals, especially in terms of less carbohydrate, may have significant effects on exercise tolerance and breathlessness amongst patients with COPD. [Diets Rich in Carbohydrates Worsens COPD, Medical Tribune, July 23, 1992; p.17]
Increased Fruit/Vegetable Consumption
A diet high in antioxidants may protect against the free-radical-damaging effect of environmental toxins or cigarette smoke. Studies comparing different populations have shown that increasing fruit consumption appears to reduce the risk of developing chronic bronchitis.
Digestive Aids
Bromelain
Bromelain has been shown to reduce cough and thin mucus secretions for easier removal in chronic bronchitis, but probably not in acute bronchitis.
Environmental
") Particulate Matter Avoidance
Particulate Matter Avoidance
Long-term effects of particulate air pollution on the incidence of bronchitis, emphysema and asthma have been documented. There is an unexpectedly high COPD mortality found in small agricultural communities, which may be in part due to occupational dust exposure. The authors felt that prevention of COPD should start in childhood, with emphasis on infection prevention and the control of indoor pollution. [Environmental Factors and Chronic Obstructive Pulmonary Disease, European Respiratory Review, 1992;2:9; pp.144-148]
Habits
Laboratory Testing
Test Antioxidant Status
Oxidative stress appears to play a role. Deficiencies of glutathione and vitamins E and C were found in patients with COPD. Increased lipid peroxidation is also a concern. [Oxidative Stress in Chronic Obstructive Pulmonary Disease, American Journal of Respiratory and Critical Care Medicine, 1997;156: pp.341-57]
Test Magnesium Levels
There is a possibility that magnesium deficiency contributes to pulmonary complications. The authors note during the past few years there has been an increase in calcium consumption in the U.S. but little change in magnesium intake, which may imbalance the calcium:magnesium ratio. Serum levels can be normal and yet there can be magnesium deficiency within cells. These authors believe pulmonary patients should be routinely monitored for magnesium deficiency. There have been noted benefits of magnesium for wheezing also. [Role of Magnesium in Regulation of Lung Function, The Journal of the American Dietetic Association, June 1993;93(6): pp.674-677]
Physical Medicine
Calming / Stretching Exercises
For those who have trouble breathing, exercise of any form might not sound like a good idea. However, exercise does help the body to use oxygen more efficiently; the key is not to overdo it. Several studies have confirmed the benefits of yoga for COPD patients. Lung function, inflammation, quality of life, and breathing all showed significant improvement.
In an experiment conducted in Western Australia, 22 male patients aged 52 to 65 were selected for severe breathing problems such as chronic bronchitis (emphysema) that made normal breathing impossible.
Half of the men underwent standard treatment for 9 months: physiotherapy that included relaxation techniques, breathing exercises and general workouts to improve stamina. The other 11 men were given a yoga teacher instead of a physiotherapist. He taught them techniques of yoga breathing, which encouraged the use of all chest and abdominal muscles as well as ten yoga postures.
The difference between the two groups was striking. The men who had practiced yoga showed a significant improvement in their ability to exercise, but the physiotherapy group did not. Eight or more out of the 11 patients who underwent yoga declared that they had definitely increased tolerance for exertion and that they recovered more quickly after exertion. The physiotherapy group reported no similar improvement. A significantly greater number of patients reported that "with the help of yogic breathing exercises, they could control an attack of severe shortness of breath without having to seek medical help", according to the study.
Doctors analyzing the results from the study postulate that, after the training, the breathing pattern of the patients in the yoga group changed to a slower and deeper cycle, allowing them to tolerate higher work loads. Patients in the physiotherapy group continued in their shallow rapid breathing pattern.
Supplements
Essential Fatty Acids
A high intake of omega-3 fatty acids may protect cigarette smokers against chronic obstructive pulmonary disease. Supplementing with omega-3 fatty acids may interfere with the inflammatory mediators triggered by cigarette smoking. Even small increments of omega-3 fatty acids may have a cumulative beneficial effect. [Dietary N-3 Polyunsaturated Fatty Acids in Smoking-Related Chronic Obstructive Pulmonary Disease, The New England Journal of Medicine, July 28, 1994;331(4): pp.228-33].
Report by The Analyst™
Click to see sample report
Click to see sample report
Health problems rarely occur in isolation or for obvious reasons
Your body is a highly complex, interconnected system. Instead of guessing at what might be wrong, let us help you discover what is really going on inside your body based on the many clues it is giving.
Our multiple symptom checker provides in-depth health analysis by The Analyst™ with full explanations, recommendations and (optionally) doctors available for case review and answering your specific questions.
KEY
Weak or unproven link:
may be a sign or symptom of; may suggest; may increase risk of
Strong or generally accepted link:
is often a sign or symptom of; often suggests

Definite or direct link:
strongly suggests; usually leads to
Strong counter-indication:
often contraindicates; often decreases risk of

Definitely or absolutely counter-indicates:
strongly contraindicates
May be useful:
may help with
Moderately useful:
often helps with
Very useful:
is highly recommended for
Last updated: Jun 13, 2021