Macular Degeneration: Overview
The macula is found at the center of the retina where the incoming rays of light are focused. The macula is responsible for what we see straight in front of us, for the detailed vision needed in activities such as reading and writing, for recognizing faces, and our ability to appreciate color.
Macular Degeneration is a condition in which the delicate cells of the macula become damaged and stop working. Vision loss usually occurs gradually and typically affects both eyes at different rates.
Diagnose your symptoms now!
- see your health summarized and in detail
- learn what you should be doing right now
- have a doctor review your case (optional)
Causes and Development; Contributing Risk Factors
The root cause of macular degeneration is unknown, but it tends to happen as people get older. There are two forms of age-related macular degeneration, namely "dry" and "wet".
The "dry" form makes up around 70% of cases: the visual cells simply cease to function, like the colors fading in an old photograph. The process involves thinning of the macular tissues and disturbances in its pigmentation.
The "wet" form makes up the remaining 30% of cases and can involve bleeding within and beneath the retina, opaque deposits, and eventually scar tissue. The "wet" form accounts for 90% of all cases of legal blindness amongst macular degeneration patients.

During the early stages of macular degeneration, central vision becomes blurred and/or distorted
The dry form will often begin to convert to wet, with the formation of abnormal choroidal blood vessels – angiogenesis. The reason why angiogenesis occurs is unknown but it is believed that this additional blood vessel development is somehow caused by deposits being left in the back of the eye. These deposits are similar to age spots on the skin. These new blood vessels are fragile and have a propensity to leak and bleed, eventually forming scar tissue and resulting in irreversible vision loss.
Different forms of macular degeneration may occur in younger patients. These non-age-related cases may be linked to heredity, diabetes, nutritional deficits, head injury, infection, or other factors.
Studies of twins indicate that both genetic and non-genetic factors play important roles in age-related macular degeneration. If several members of a family are sufferers then it is very important that other members have their eyes checked regularly. Inherited macular degeneration is known as macular dystrophy.
Any type of smoking or exposure to tobacco smoke can accelerate the development of the "wet" type of macular degeneration.
Signs and Symptoms
The formation of new blood vessels and yellow deposits ("drusen") in and under the macula is often the first physical sign that macular degeneration may develop.

In advanced macular degeneration, a blank or dark area develops in the center of vision, leaving only peripheral vision
In the early stages, central vision becomes blurred or distorted, with objects having an unusual size or shape. This may happen quickly or develop over several months. The patient may be very sensitive to light or actually see lights that are not there.
Those with the advanced condition will often notice a blank patch or dark spot in the center of their sight. This makes activities like reading, writing, driving and recognizing small objects or faces very difficult.
The following are NOT known to be linked to macular degeneration: floaters (moving spots caused by debris floating in the vitreous fluid between the lens and the retina); dry eye syndromes; cataracts and cataract surgery.
Peripheral vision (side vision) isn't affected by macular degeneration.
Diagnosis and Tests
Some cases of age-related macular degeneration are detected early during a routine eye test. It will often be suspected in those aged over 60 who are experiencing changes in their central vision.
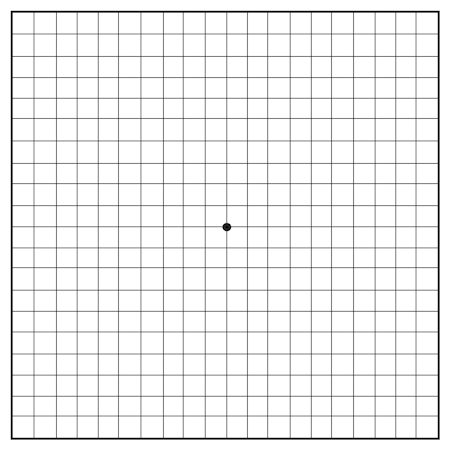
Amsler grid eye test: Cover one eye and look at the dot in the center. Note any blurry, distorted, broken or missing lines.
The following tests may be performed:
- Visual acuity test – how well the patient can see at various distances
- Dilated eye exam – eye drops are used to widen the pupils before looking for signs of macular degeneration
- Tonometry – to measure the pressure inside the eye
- The Amsler Grid – viewing a simple black-and-white grid with a dot at the center to see if areas on the grid are distorted, blurry, or discolored.
Early detection is important because a patient destined to develop macular degeneration can sometimes be treated before symptoms appear and this may delay or reduce the severity of the disease. Furthermore, as we develop better treatments for macular degeneration, whether they are medicinal, surgical, or low vision aids, those patients diagnosed with macular degeneration can sooner benefit from them.
Treatment and Prevention
At this time there is no known cure for macular degeneration. There are ways to slow macular degeneration, depending on the type and the degree of the condition. Current treatments fall into three main categories:
- Nutritional Intervention
Surgery. Laser surgery to remove the scar produced by macular degeneration has been successful in about 10% of people with disciform degeneration, mainly the younger patients. If the degeneration is associated with leaking blood vessels in the center of the macula and vision is worse than 20⁄70 then laser surgery called photocoagulation is recommended. This will not improve vision but generally reduces further vision loss. Unfortunately for most people, the area of degeneration is in the middle of the macula, at its focal point. This means that treatment cannot be given because the scars produced by the laser would make central vision worse rather than better. 'Dry' degeneration cannot be treated by laser.
Retinal transplantation is a new experimental approach to macular degeneration, but will require research to determine its safety and effectiveness.
- Making the most of remaining vision. Low vision aids (such as brighter reading lights, magnifying glasses and more sophisticated devices) and techniques for maximizing the use of peripheral vision are used to help patients adapt better to their loss of central vision.
Special sunglasses that block out the blue end of the spectrum may decrease the progress of the disease. It has been demonstrated that the blue rays of the light spectrum seem to accelerate macular degeneration more than the others. This means that very bright light, such as sunlight or its reflection in the ocean and desert, may worsen macular degeneration.
Although the medications used to treat hypertension have not been shown to have any direct effect on macular degeneration, they may slow progression of the disease by reducing hypertension. Hypertension tends to make some forms of macular degeneration worse, particularly in the "wet" form where the retinal tissues are invaded by new blood vessels.
Prognosis; Seek medical attention if...
There is some good news: macular degeneration is not painful, and never leads to total blindness. It is the most common cause of poor sight in people over 60 but never leads to complete sight loss because it is only the central vision that is affected. Macular degeneration never affects vision at the outer edges of the eye, so most sufferers will have enough side vision to get around and keep their independence.
The bad news is that if you have macular degeneration in one eye then it will usually develop in the other also. In the early stages, only one eye may be affected, but as the disease progresses, both eyes are usually affected. Even with a loss of central vision, however, color vision and peripheral vision may remain clear.
In some cases, macular degeneration may be active and then slow down considerably, or even stop progressing for many years.
The following signs may be indicative of macular problems and anyone experiencing these symptoms should consult an ophthalmologist immediately:
- The major risk factors: aging, atherosclerosis and hypertension
- Straight lines appear distorted and, in some cases, the center of vision appears more distorted than the rest of the scene
- A dark, blurry area or "white-out" appears in the center of vision
- Color perception changes or diminishes
On This Page
Macular Degeneration:Signs, symptoms & indicators of Macular Degeneration:
Symptoms - Head - Eyes/Ocular
 vision disturbances is often a sign or symptom of Macular Degeneration") (Severe) vision disturbances
(Severe) vision disturbances
In the early stages, central vision may be blurred or distorted, with things looking an unusual size or shape. This may happen quickly or develop over several months.
 sensitivity to bright light may be a sign or symptom of Macular Degeneration") (High) sensitivity to bright light
(High) sensitivity to bright light
Those suffering from macular degeneration may be very sensitive to light or actually see lights that are not there.
Conditions that suggest Macular Degeneration:
Symptoms - Head - Eyes/Ocular
Risk factors for Macular Degeneration:
Addictions
Cigarette Smoke Damage
Any type of smoking or exposure to tobacco smoke can accelerate the development of the 'wet' type of macular degeneration. Smokers on average exhibit only half the density of yellow macular pigment (lutein and zeaxanthin) and develop macular degeneration 7 years sooner than non-smokers.
Family History
Macular degeneration in family
Children and young people can suffer from an inherited form of macular degeneration called macular dystrophy. Sometimes several members of a family will suffer from this, and if this is the case in your family it is very important that you have your eyes checked regularly.
Supplements, Medications, Drugs
Frequent aspirin use
A study published in October 2011 and involving 4,000 elderly participants across Europe found that those who took aspirin every day were twice as likely to be diagnosed with late stage age-related macular degeneration (AMD) as those who did not.
NOTE: For those suffering from heart disease, the benefits of taking aspirin outweigh the risks posed to their vision.
During another major study at the Netherlands Institute for Neuroscience and Academic Medical Centre, researchers followed 839 people and found that among those who took aspirin each day, around 4% had an advanced form of the disease called neovascular or 'wet' AMD, which leads to the most profound blindness. In comparison, just 2% who took aspirin less frequently had the same disease.
A more conclusive Australian study was published January 2013 in the Journal of the American Medical Association (JAMA) and followed 2,400 subjects for 15 years. It found that 3.7% of the 'occasional' users of aspirin and 9.4% of the 'regular' users developed wet AMD.
Counter-indicators
 Much/some B-complex supplementation
Much/some B-complex supplementation
Harvard University researchers found that the B vitamins protect our eyes. Those taking daily B6, B9 (folic acid) and B12 supplements had a significantly reduced risk of developing age-related macular degeneration.
Concerned or curious about your health? Try The Analyst™

Symptom Entry

Diagnosis

Suggestions

LifeMeter®

Explanations

Review (optional)
Recommendations for Macular Degeneration:
Amino Acid / Protein
 L-Glutathione
L-Glutathione
Researchers have found that age-related macular degeneration correlates with low glutathione levels. When taking into consideration other variables such as smoking, age, cardiovascular disease and multivitamin use, depletion of glutathione by itself was thought to be a major contributing factor behind macular degeneration. [British Journal of Ophthalmology, 1994; 78 [10], pp.791-4)]
Botanical / Herbal
Bindweed
Bindweed prevents new vessel growth and may help stop the scarring and permanent damage seen with wet macular degeneration. The suggested dose is two 250mg capsules per day.
 Ginkgo Biloba
Ginkgo Biloba
Ginkgo Biloba appears to reduce the risk of macular degeneration. [Recent Results in Pharmacology and Clinic, Fuenfgeld FW, ed. Berlin: Springer-Verlag, 1988; pp.231-6]
Diet
Increased Fruit/Vegetable Consumption
There is evidence that eating fresh fruits and dark green, leafy vegetables (such as spinach and collard greens) may delay or reduce the severity of age-related macular degeneration.
 Low/Decreased Fat Diet
Low/Decreased Fat Diet
Some scientists have suggested an association between macular degeneration and high saturated fat, low carotenoid pigments, and other substances in the diet.
Mineral
Zinc
Oral use of zinc has produced improvement in vision. Intravenous administration along with selenium have demonstrated benefits in the treatment of macular degeneration. According to researchers at Harvard University, however, zinc has shown mixed results. [Arch Ophthalmol 1988:106, pp.192-8]
Selenium
Selenium is sometimes recommended, but you should always consult your physician to determine appropriate dosages.
Supplements
Vitamins
Preventive measures against Macular Degeneration:
Botanical / Herbal
Bilberry
Bilberry contains compounds which act as antioxidants in the retina, making it a possible preventive measure for macular degeneration [Klin Monatsbl Augenheilkd Beih 1981;178: pp.386-9]. It also strengthens capillaries in the retina and reduces hemorrhaging [Minerva Med 1977;68: pp.3565-81]. An oral dose is in the range of 40 to 80mg (24% anthocyanosides) per day.
Supplements
Lutein
Lutein, an antioxidant found in spinach and kale, works extremely well in protecting the retina against sunlight damage [Methods Enzymol 1992:213: pp.360-6]. Supplementation with 6mg of Lutein daily may decrease the occurrence of macular degeneration by more than 50% [JAMA 1994:272: pp.1413-20]. Lutein is one of the primary antioxidants for the macula rather than for the lens of the eye.
Vitamins
Vitamin C (Ascorbic Acid)
Taking anti-oxidants such as vitamins C and E has beneficial protective effects against age-related macular degeneration (AMD). Since oxidative damage of the eye can cause macular degeneration, taking antioxidants may lower the disease's occurrence. People with high levels of vitamin C, vitamin E and selenium appear to have a 70% lower risk of developing macular degeneration. [Arch Ophthalmol, December 1995:113(12, 15): pp.18-23; Arch Ophthalmol 1993:111: pp.104-9]
Long-term use of multiple antioxidants plus zinc and copper clearly reduced the risk of developing advanced AMD and the rate of visual acuity loss in a randomized, double-blind, placebo-controlled trial of 3,640 older adults (aged 55-80 years) with preexisting retinal abnormalities, advanced AMD or vision loss due to AMD who were followed for an average of 6.3 years. [AREDS Report No. 8. Arch Ophthalmol 2001;119(10): pp.1417-1436]
Report by The Analyst™
Click to see sample report
Click to see sample report
Health problems rarely occur in isolation or for obvious reasons
Your body is a highly complex, interconnected system. Instead of guessing at what might be wrong, let us help you discover what is really going on inside your body based on the many clues it is giving.
Our multiple symptom checker provides in-depth health analysis by The Analyst™ with full explanations, recommendations and (optionally) doctors available for case review and answering your specific questions.
KEY
Weak or unproven link:
may be a sign or symptom of; may increase risk of
Strong or generally accepted link:
is often a sign or symptom of; often increases risk of; often leads to

Definite or direct link:
is a sign or symptom of; strongly suggests
Weakly counter-indicative:
may decrease risk of
May be useful:
may help with; may help prevent
Moderately useful:
often helps with; often prevents
Very useful:
is highly recommended for
Last updated: May 20, 2024