Urinary Tract Infection (UTI): Overview
Alternative names: Acute cystitis, Simple cystitis, Bladder infection, Symptomatic bacteriuria
Occurring in otherwise healthy individuals with no neurological or structural abnormalities, acute, symptomatic, uncomplicated urinary tract infection (UTI) may be the most common infection after the common cold and flu. Most UTIs are bladder infections.
Diagnose your symptoms now!
- let The Analyst™ find what's wrong
- check your overall health status
- have a doctor review your case (optional)
Natural Defense Mechanisms. The greatest defense mechanism against bacterial inflammation and adherence to the bladder or urethral lining is urine: invading bacteria stimulate urination. Voiding washes out bacteria from the bladder and urethra and dilutes bacterial concentrations, preventing adherence.
The surface cells of the bladder are coated with a special urinary mucus. This thin negatively-charged surface layer attracts water molecules and forms a barrier between the bladder and urine, preventing bacterial adherence. White blood cells will also move into the bladder and urine to kill the invading bacteria. The kidneys produce a protein which contains mannose residues that block the attachment points of some types of E. coli. This prevents their attachment to the bladder and encourages their excretion.
Incidence; Causes and Development; Contributing Risk Factors
Acute bacterial cystitis affects 8-10 million Americans each year. An acute UTI will be experienced by 25 to 40% of females in their lives, and up to 6% of women will have one or more UTIs in a given year.
Cystitis is a common occurrence in women, but it is less common and a potentially more serious condition for men.
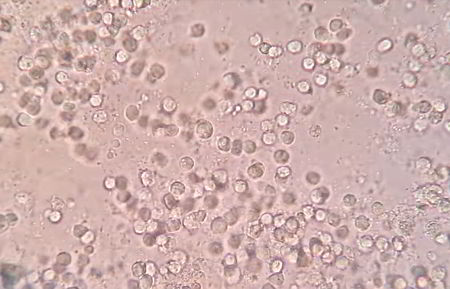
Pus cells, red blood cells, and bacteria in the urine of a female UTI patient, seen through a microscope
E. coli is responsible for more than 80% of all acute female bladder infections. However, S. saprophyticus is more often isolated from women using spermicide-coated condoms (74%) and diaphragms than is E. coli. Other bacteria such as Proteus, Klebsiella or Enterobacter are occasionally isolated from uncomplicated UTIs. Vaginitis and urethritis caused by sexually transmitted pathogens such as herpes simplex, chlamydia or gonorrhea may mimic cystitis.
For men the cause can be an underlying bladder or prostate infection, an obstruction or tumor, or an enlarged prostate.
The largest risk factor for acquiring and developing an acute UTI is being female. This is because the short female urethra provides greater access to the bladder, and the nearby vagina provides a favorable environment for bacterial colonization and growth.
The risk of acquiring an acute infection is more than 3-fold among women with a previous infection compared to women with no history of UTI.
Sex and Cystitis
Once referred to as "honeymoon-cystitis", many women acquire their first infection after their first sexual experience. A study has shown that, compared to women who have not been sexually active during the previous week, the relative risk of a UTI among unmarried women increases 2.6 times for women who have engaged in sexual intercourse 3 times per week, and 9.0 times for women who have had intercourse seven times during the previous week. New sex partners and intercourse methods introduce bacteria into the vagina and urethral area. If bacteria are not removed by voiding or cleaning, they will colonize in this area, posing a risk of infection.
Barrier methods of birth control can also increase the risk of acquiring a UTI. Condoms increase the risk of vaginal tears, allowing bacteria to invade and adhere. Contraceptive sponges, foams, creams, gels and condoms use nonoxynol-9 (N-9) as a spermicide. Lactobacilli, the normal flora of the vagina, provide protection from external bacteria overgrowth, but are eradicated by N-9. The removal of lactobacilli by N-9 or other antibiotics alters the vaginal pH and natural flora, allowing Escherichia coli (E. coli) and Staphylococcus saprophyticus to proliferate, colonize and adhere to the vaginal mucosa. The odds that a woman exposed to condoms coated with N-9 would get a UTI were found to be 3 times higher than for sexually active women who did not use coated condoms. Diaphragms that are worn for more than 24 hours or improperly fitted can harbor bacteria or irritate tissue. A cervical cap, however, may not be associated with an increased UTI risk; less spermicide is used inside the enclosed cap, causing less alteration of the vaginal flora. Using extra lubricant during sex to decrease friction and irritation can help prevent the development of an infection.
Signs and Symptoms
Signs and symptoms of a complicated infection include nausea, vomiting, flank pain, fever and chills. Treatment may require hospitalization and longer, more expensive antibiotic treatment.
Diagnosis and Tests
As a man, if you experience the symptoms of cystitis, you should see your doctor immediately. An analysis and culture/sensitivity of your urine will be performed which should identify the kind of bacteria causing the infection and the antibiotic most likely to help.
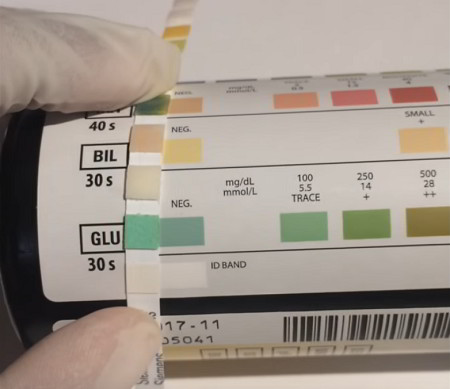
A positive urine dipstick test for leukocyte esterase normally indicates the presence of bacteria
The leukocyte esterase (LE) dipstick test is used to screen for pyuria (presence of pus in the urine when voided). LE, an enzyme found in neutrophil granules, reacts with an impregnated reagent pad to produce a blue color within 2-5 minutes. A positive test indicates the presence of white blood cells (WBC). When compared to standard methods of defining UTIs (isolating >=105 CFU/mL of pathogenic bacteria) or significant pyuria (>=10 WBC/mm3 urine) the sensitivity is 75%-96% and the specificity is 94%-98%. Pyuria indicates inflammation and not necessarily an infection. This is an efficient, cost-effective method for determining the presence of pyuria when routine microscopy is unavailable, impractical or for an outpatient evaluation. Vitamin C and phenazopyridine may cause false-negative or unreadable results.
The nitrate test is also widely available, for use at home or in the office. The nitrate test is qualitative in that it is used as a surrogate to detect Gram-negative bacteria, since only Gram-negative bacteria are able to produce nitrate. An aromatic amine-impregnated pad produces an azo color within 60 seconds if urinary nitrites are present. Urinary nitrites are produced by the action of Gram-negative bacteria (Enterobacteriaceae) metabolism on dietary nitrates through nitrate reductase. False-negatives can result from recent antibiotic therapy, low urinary pH (as occurs with high doses of ascorbic acid), lack of dietary nitrates, or when diuresis has created insufficient urinary nitrate levels. False-negatives also occur when Pseudomonas sp. or Gram-positive bacteria such as Staphylococcus sp., or Enterococcus sp., which lack nitrate reductase, are unable to produce nitrite. Sensitivity of the test ranges between 35%-85%, and the specificity ranges between 92%-100%.
Treatment and Prevention
When promptly treated, the period of discomfort can be shortened and the potential for more serious damage and recurrence is reduced. Treatment is usually recommended because if the infection progresses and spreads to the kidneys it is then classified as a complicated infection.
In the past, the treatment of acute female cystitis with an antibiotic for 7-14 days was the standard procedure. Although very effective, the associated adverse events, poor compliance and unnecessary costs necessitated a re-evaluation. Single-dose therapy is generally less effective than the same antimicrobial used for 7-14 days, but most antimicrobials given for three days are as effective as the same antimicrobial given for 7-14 days.
Complications
Cystitis in men is not serious if treated promptly, but the discomfort can be chronic and disabling. Untreated bladder infections can cause kidney or prostate infections and damage.
On This Page
Urinary Tract Infection:Signs, symptoms & indicators of Urinary Tract Infection (UTI):
Symptoms - General
Symptoms - Urinary
 painful urination is often a sign or symptom of Urinary Tract Infection (UTI)") (Slightly/very) painful urination
(Slightly/very) painful urination
Symptoms include painful, burning or itching sensations during urination.
Counter-indicators
Risk factors for Urinary Tract Infection (UTI):
Autoimmune
") Lupus, SLE (Systemic Lupus Erythematosus)
Lupus, SLE (Systemic Lupus Erythematosus)
Infections of the urinary tract are common in lupus patients.
Hormones
Progesterone Excess
One mysterious effect in the progesterone intolerant women is bladder problems. Some women have either a great increase in urinary tract infections or a feeling like they are having an infection as soon as they try taking a "normal" progesterone dose. If bladder symptoms start and stop with starting and stopping progesterone, they may be related.
Nutrients
Vitamin A Requirement
Retinoic acid (an analogue of vitamin A) is needed for the differentiation of basal cells into mucus epithelial cells. A deficiency results in keratinization of mucus membranes that line the respiratory tract, intestines, urinary tract and epithelium of the eye. This in turn decreases the protective barrier role played by these membranes, resulting in an increased number of infections and other pathologies.
Concerned or curious about your health? Try The Analyst™

Symptom Entry

Diagnosis

Suggestions

LifeMeter®

Explanations

Review (optional)
Urinary Tract Infection (UTI) could instead be:
Female-Specific
Urinary
Interstitial Cystitis
Interstitial cystitis and urinary tract infections have similar symptoms, but interstitial cystitis tests negative for bacteria.
Recommendations for Urinary Tract Infection (UTI):
Botanical / Herbal
") Cranberry Juice
Cranberry Juice
There is evidence to suggest that drinking cranberry juice in addition to water can help fight a bladder infection. Since the mid-1800s, cranberry juice has been associated with urinary antibiotic properties. The juice does not appear to work by acidifying the urine, but rather contains compounds that have a mild antibacterial quality or help prevent E. coli from adhering to tissues. There is evidence that if you consume a glass of cranberry juice each day, it could reduce the incidence of urinary tract infections (UTI).
It has been reported that cranberries contain more mannose than any other food. This sugar, D-mannose, blocks E. coli attachment. Since the mannose content in cranberries is relatively low, many natural doctors now use supplemental D-mannose to deal with the most common form of cystitis, an E. coli infection. D-mannose can be used for preventive purposes also.
A study was conducted at the Finnish Student Health Services at Oulu University with 150 women with persistent UTIs. Fifty drank 50ml (just under 2oz) of cranberry juice concentrate per day for six months. Another 50 drank a preparation of Lactobacillus, while the final 50 women were given no treatment. After six months, only eight women taking cranberry juice had experienced a UTI, compared with 19 of those taking Lactobacillus, and 18 not taking anything.
For prevention, a widely-accepted dose is 3 ounces (90ml) of 33% pure cranberry juice daily to prevent an infection and 12-32 ounces (350-950ml) per day for treatment. 50ml of cranberry juice concentrate is well-tolerated and is also effective in preventing bladder infections. Larger quantities should be considered when an infection is present. Note that supermarket cranberry cocktail or juice may be very diluted and may produce no benefit if not taken in sufficient quantities to approximate a 50ml dose of concentrate. Check labels to ensure a high proportion of actual cranberry juice in whatever preparation you choose, or use only concentrate or powder forms.
Diet
Increased Water Consumption
The mainstay of prevention is to keep the urine dilute by drinking fluids and urinating often. Added water consumption during an infection will help flush out the problem bacteria. Repeated infections may require that routine water consumption be increased to prevent their recurrence.
") Caffeine/Coffee Avoidance
Caffeine/Coffee Avoidance
Coffee, soda and other caffeinated beverages may irritate the bladder lining and are not recommended.
Drug
Antibiotics
While natural means may prevent as well as treat cystitis, there are times when the judicious use of antibiotics is the best treatment choice. Natural means alone will often prevent recurrence and in some cases resolve bladder infections that have resisted antibiotic treatment.
Hormone
Laboratory Testing
Urinalysis
Urine culture and susceptibility testing add little to the eventual choice of an antibiotic as treatment because of the limited number of possible pathogens. Many patients, therefore, may receive an abbreviated laboratory work-up using dipstick tests to screen for the presence of bacteria and white blood cells.
If treatment does not improve symptoms, further testing should be done. Cultures need to be performed when the diagnosis is unclear or when there are other risk factors such as a history of recurrent infections. Cultures should also be performed when symptoms such as fever, lower back pain or signs associated with vaginitis are present.
During urinalysis, urine pH is determined. If elevated, lowering it will assist in resolving the infection.
Mineral
Physical Medicine
Not recommended
Vitamins
Vitamin C (Ascorbic Acid)
The urine pH is often elevated in times of bacterial infection but can be lowered by some medications or unbuffered vitamin C. This produces a less favorable growth environment for some bacteria.
Preventive measures against Urinary Tract Infection (UTI):
Habits
Personal Hygiene Changes
For women, poor personal hygiene following urination or defecation can expose the vagina and urethra to bacteria from the surrounding area. To prevent bladder infections, practice good personal hygiene by always "wiping front to back" to keep bacteria from entering and colonizing the vagina and urethra. Wash the skin around the vagina, perineum and rectum daily. Shower or bathe but avoid bubble baths, bath oils and scented soaps, which can act as irritants. During menstruation, change sanitary pads every 2-3 hours and tampons every 4-5 hours. Sanitary pads and tampons containing deodorants or perfumes can irritate the skin, allowing bacteria to enter.
Report by The Analyst™
Click to see sample report
Click to see sample report
Health problems rarely occur in isolation or for obvious reasons
Your body is a highly complex, interconnected system. Instead of guessing at what might be wrong, let us help you discover what is really going on inside your body based on the many clues it is giving.
Our multiple symptom checker provides in-depth health analysis by The Analyst™ with full explanations, recommendations and (optionally) doctors available for case review and answering your specific questions.
KEY
Weak or unproven link:
may be a sign or symptom of; may increase risk of; is very occasionally misdiagnosed as
Strong or generally accepted link:
is often a sign or symptom of

Definite or direct link:
is a sign or symptom of

Strong counter-indication:
often contraindicates

Definitely or absolutely counter-indicates:
strongly contraindicates

May be useful:
may help with
Moderately useful:
often helps with
Very useful:
is highly recommended for; usually prevents

Often counterindicated:
is often not recommended for
Last updated: Jun 04, 2020