Osteoarthritis: Overview
Alternative names: Wear-and-tear arthritis, Degenerative joint disease, Degenerative arthritis
Osteoarthritis (OA) is a chronic disease in which cartilage breaks down over time, causing pain, inflammation and stiffness in the joints. It is by far the most common form of arthritis. Nearly all vertebrates suffer from OA, including porpoises and whales, and those long-extinct giants, the dinosaurs.
Diagnose your symptoms now!
- see your health summarized and in detail
- have a doctor review your case (optional)
- identify any nutritional deficiencies
Cartilage is the slippery tissue that covers the ends of bones in a joint, allowing the bones to glide over one another. It also absorbs energy from the shock of physical movement. When cartilage in a joint deteriorates, Osteoarthritis occurs.
There are two types of Osteoarthritis: primary and secondary. Primary OA appears without any apparent cause, usually as a result of aging. Secondary OA occurs in joints that have sustained injuries, or experienced infections or fractures.
Incidence; Causes and Development
Some facts:
- Osteoarthritis affects about 1-in-15 Americans
- The World Health Organization estimates that 1-in-4 of the world's population over 65 suffers from OA
- OA is 8 times more common than rheumatoid arthritis (RA)
- Almost everyone over the age of 75 is affected in at least one joint
- Before age 45, more men have it; after age 45, it is more common in women
- OA places a high economic burden on society through disability, related disease, and the high cost of treatment
The pain of Osteoarthritis is often caused by ligament relaxation around the joint: old cartilage breakdown exceeds new cartilage synthesis, leading to loose ligaments and joint instability.
Secondary OA can be caused by obesity (added pressure on weight-bearing joints), or as the result of another type of arthritis, such as rheumatoid arthritis.
Signs and Symptoms
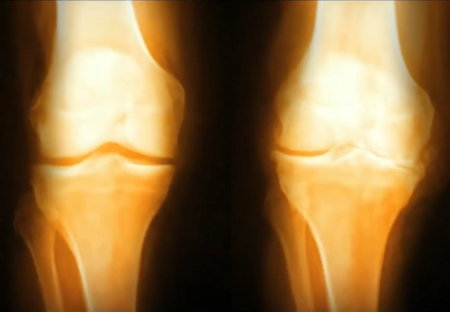
The joint space in a normal knee (left) compared to an osteoarthritic knee where bones rub together due to loss of cartilage
As the cartilage in a joint deteriorates, the bones begin to rub together, causing pain, swelling, and loss of motion of the joint. The joint may begin to lose shape. Small bone spurs called osteophytes may grow on the edges of the joint. Inflammation may or may not be present. The pain may come and go. These symptoms almost always begin gradually, taking years until the pain is severe enough to be reported to a doctor. OA is commonly found in the joints of the fingers, feet, knees, hips and spine, and is rarely found in joints of the wrist, elbows, shoulders or jaw.
Diagnosis and Tests
Although it is usually not difficult to diagnose OA, no single test can pinpoint the disease. Most doctors use a combination of patient history, physical examination and X-rays to diagnose the disease and rule out other causes for the symptoms.
Treatment and Prevention
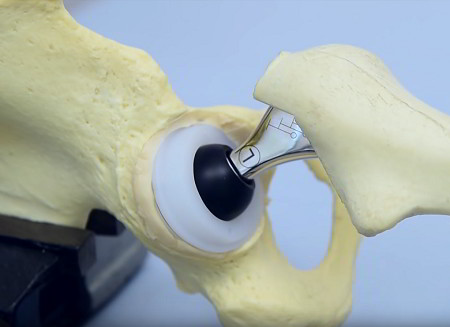
An artificial hip joint, with ball cemented into the end of the femur (right) and socket cemented into the original socket
Hip and knee replacement surgery (arthroplasty) is a very common and successful procedure for those with joint damage and pain that interferes with normal activities.
Treatment of Osteoarthritis should focus on managing pain while improving joint function by strengthening the joint and encouraging cartilage growth. This can be done in several ways.
People in occupations or activities requiring repetitive and stressful movement should find ways to reduce joint trauma. Adjusting the work area, substituting tasks or changing exercise activities to produce less stress on joints can help reduce further 'wear and tear'.
Corticosteroids are typically injected into affected joints rather than taken orally to relieve the pain, but repeated injections may further weaken loose ligaments and prevent healing which requires an inflammatory like response.
Maintaining the structural integrity of the synovial joints is fundamental to osteoarthritis prevention.
Complications
Osteoarthritis leads to rapid and complete breakdown of cartilage. Those affected have increased risk of developing bone death (osteonecrosis), stress fractures, bleeding inside the joint, gout, poor sleep quality, weight gain due to inactivity, chondrocalcinosis (calcium crystals in the joints), anxiety, depression, deterioration of tendons and ligaments, pinched nerves in the spine, disability and reduced productivity.
On This Page
Osteoarthritis:Signs, symptoms & indicators of Osteoarthritis:
Symptoms - Environment
 (Minor/major) pain in cold/cool/damp weather
(Minor/major) pain in cold/cool/damp weather
Like all arthritic conditions, osteoarthritis can react to weather changes: good weather can ease pain, and cold, damp weather can make it worse.
Counter-indicators
 No pain in cold/cool/damp weather
No pain in cold/cool/damp weather
Like all arthritic conditions, osteoarthritis can react to weather changes: good weather can ease pain, and cold, damp weather can make it worse.
Symptoms - Skeletal
 Morning stiffness that eases rapidly or variable duration morning stiffness
Morning stiffness that eases rapidly or variable duration morning stiffness
Osteoarthritis patients' symptoms typically improve within 30 minutes but may be aggravated during the day with use of the affected joints.
 non-specific arm pain may be a sign or symptom of Osteoarthritis") (Severe) non-specific arm pain
(Severe) non-specific arm pain
Degenerative wear and tear may affect the ligaments and musculature surrounding the elbow, resulting in chronic diffuse arm pain or pain that is poorly defined about the elbow.
Conditions that suggest Osteoarthritis:
Musculo-Skeletal
Heberden's Nodes
The symptoms of osteoarthritis usually begin slowly and may be mild at first. The pain is usually worse after a lot of activity or during movement after long periods of inactivity. You may feel discomfort in the joint before or during a change in the weather. You may also have swelling and loss of flexibility in the joint. Over time, the cartilage that serves as a cushion between the bones may completely wear away, causing the bones to rub against each other. This can cause the bone ends to thicken and form bony growths or spurs. In the fingers these bony lumps are called Bouchard's or Heberden's nodes.
TMJ Problems
The TMJ may be affected by osteoarthritis, usually in those over 50 years old. Symptoms include stiffness, grating, or mild pain. Both sides of the jaw are usually involved.
Symptoms - Skeletal
Concerned or curious about your health? Try The Analyst™

Symptom Entry

Diagnosis

Suggestions

LifeMeter®

Explanations

Review (optional)
Risk factors for Osteoarthritis:
Metabolic
Problems Caused By Being Overweight
Forcing joints to carry more weight than they were designed for often results in premature failure.
Symptoms - Muscular
Having excess body fat
Extra weight contributes to the wear-and-tear and gradual breakdown of the hips, knees, and feet. There is also evidence that extra fats play a part in the degeneration of joint cartilage.
Counter-indicators
Being very skinny or being lean or underweight
Being thin or underweight permits fluid movement of the joints and means they don't take such a pounding as they do when we are overweight. Relatively few of those needing hip and knee replacements are slim.
Osteoarthritis suggests the following may be present:
Habits
The Effects Of Overtraining
Cortisol – a hormone produced by the adrenal gland during periods of intense physical exercise – interferes with bone-building and reduces bone density by breaking down bone faster than it is made.
Hormones
Estrogens Low
In studies of older women, a lower risk of osteoarthritis was found in women who had used oral estrogens for hormone replacement therapy. The researchers suspect that low estrogen levels could increase risk for the disease, but further studies are needed.
Nutrients
Manganese Requirement
Bone cartilage can't grow or repair itself adequately without manganese – an essential part of glucosamine, which is in turn a major joint building block. When glucosamine is in short supply, various forms of arthritis tend to arise, eventually leading to joint deterioration.
Recommendations for Osteoarthritis:
Amino Acid / Protein
 L-Phenylalanine
L-Phenylalanine
D-phenylalanine (DPA) has been used to treat the chronic pain of osteoarthritis with both positive and negative results.
Animal-derived
 Glucosamine / Chondroitin Sulfate
Glucosamine / Chondroitin Sulfate
Clinical studies comparing glucosamine (in sulfate or hydro-chloride form) with both placebo and standard arthritis drugs (including Ibuprofen) have shown that glucosamine outperformed both in reducing long-term pain, joint tenderness and swelling, accelerating recovery, reversing cartilage damage, and helping to restore joint function, range of motion, and walking speed. Glucosamine is a component of hyaluronic acid which has been used by injection to successfully reduce knee pain.
Three years of treatment with glucosamine sulfate (1500mg per day) prevented joint space narrowing and reduced pain in two randomized, double-blind, placebo-controlled trials with a total of 414 women, including 319 of postmenopausal age.
[North American Menopause Society 12th Annual Meeting, Oct. 4-6, 2001, New Orleans, LA.]
Along with glucosamine, chondroitin sulfate has become a widely used dietary supplement for treatment of osteoarthritis. Due to the popularity of the glucosamine-chondroitin supplement and the lack of reliable information about its usefulness in treating osteoarthritis [McAlindon TE et al (2000); Glucosamine and Chondroitin for Treatment of Osteoarthritis: A Systematic Quality Assessment and Meta-analysis; JAMA 283: pp.1469-1475.] the National Institutes of Health funded a study to test the effects of chondroitin and glucosamine on osteoarthritis of the knee.
This multicenter, placebo-controlled, double-blind, six month long trial found that glucosamine plus chondroitin had no statistically significant effect on symptoms of osteoarthritis.[Clegg DO et al (2006); Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis; New Engl J Med 354 (8): pp.795-808.]
The control group of patients who took celecoxib (a commonly used osteoarthritis drug) did have a statistically significant improvement in their symptoms. These results indicate that glucosamine and chondroitin do not effectively relieve osteoarthritic pain. Although the study found no overall effect for the supplements, a secondary analysis of a subgroup of patients suggested that the supplements taken together helped people with more severe pain.
Botanical / Herbal
Rose Hip
May 19, 2008: Scientists have found that powder made from a wild variety of rosehip, Rosa canina, is better at reducing the pain of osteoarthritis than paracetamol.
A review of studies, published in the medical journal, Osteoarthritis and Cartilage, looked at the effect of the powder on more than 300 patients who were given different pain-relieving medications for an average of three months. They found that rosehip was almost three times more effective than standard paracetamol at relieving pain. It was also almost 40% more effective than another common therapy, the drug glucosamine. Rosehip powder also did not have the side-effects associated with other pain medications, including constipation and drowsiness.
It is believed that the powder works by also tackling the inflammation associated with osteoarthritis.
 Ginger Root
Ginger Root
A concentrated extract of 2 ginger species (255mg bid) over a period of 6 weeks reduced pain in a double-blind, placebo-controlled study of 261patients with moderate to severe pain from osteoarthritis of the knee. Acetaminophen was allowed to be used if the pain was not controlled sufficiently. [Arthritis Rheum 2001;44(11): pp.2531-2538]
Boswellia
Boswellin is the first herbal remedy to have documented clinical evidence that it is useful in rheumatoid arthritis, osteoarthritis, low back pain, soft tissue rheumatism and myositis symptoms.
Chinese Medicine
Acupuncture
Some people have found pain relief using acupuncture. Preliminary research shows that acupuncture may be a useful part of an osteoarthritis treatment plan.
Diet
Weight Loss
Overweight people can lessen the shock to their joints by losing weight. Knees, for example, sustain an impact three to five times the body weight when descending stairs. Therefore a loss of five pounds can eliminate at least 15 pounds of stressful impact on the joint. The greater the weight loss, the greater the benefit.
Nightshade Family Food Avoidance
Elimination of nightshade family foods does not help all people with arthritis, but people who respond are usually helped a great deal.
Drug
NSAIDs
NSAIDs (Nonsteroidal Anti-Inflammatory Drugs) are commonly used to treat osteoarthritis. Available over the counter or by prescription, they fight inflammation or swelling and relieve pain. Acetaminophen such as Tylenol can also be very effective in treating the pain. Research has shown that in many patients acetaminophen relieves pain as effectively as NSAIDs. These pain killers will only help control the symptoms, and if used at all should only be used for pain control while more effective therapies are at work. The newer COX2 inhibitors will have fewer side effects, but still do not restore normal function. Topical pain-relieving creams, rubs and sprays can be applied directly to the skin. There are many brands available over the counter.
Habits
Aerobic Exercise
Research shows that a good treatment for Osteoarthritis is exercise. It can improve mood and outlook, decrease pain, increase joint flexibility, improve the heart and blood flow, maintain or decrease weight, and promote general well being. The amount and form of exercise will depend on which joints are involved, how stable the joints are, and whether a joint replacement has already been done.
Hormone
Invasive / Surgery
Prolotherapy
Prolotherapy is the best and often only treatment when ligaments are weakened and cartilage damaged. As good as some of the other treatments are for pain, nothing seems to come close to the effectiveness of Prolotherapy. Prolotherapy is the only treatment that can stimulate the regrowth of the injured tissue.
Hyaluronic Acid
The use of hyaluronic acid (HA) in osteoarthritis has been found to be effective in terms of relieving pain due to osteoarthritis (OA) of the knee and may potentially be a structure-modifying drug. Results of a study of 100 patients with OA of the knee who were treated with five weekly injections of intra-articular HA demonstrated significant improvement in terms of pain on walking at week five, which persisted for six months in two-thirds of patients. [Rheumatology 1999; 38: pp.602-607]
These treatments, called viscosupplementation, are administered as a course of injections into the knee joint and are believed to supplement the viscosity of the joint fluid, thereby lubricating the joint, cushioning the joint, and producing an analgesic effect. It has also been suggested that hyaluronan has positive biochemical effects on cartilage cells. However, some placebo controlled studies have cast doubt on the efficacy of hyaluronan injections, and hyaluronan is recommended primarily as a last alternative to surgery.
Mineral
MSM (Methyl Sulfonyl Methane)
Research at the UCLA School of Medicine found an 82% reduction in pain after 6 weeks of MSM use in a double-blind study on degenerative arthritis. The study lasted 4 months and involved 16 patients on about 2gm MSM per day; 10 patients on MSM and 6 on placebo. After only 6 weeks, those patients using the MSM experienced better than 80% control of their pain, while those on the placebo experienced 18% improvement. [Federation of American Societies for Experimental Biology, 69th Annual Meeting, Apr. 21-26, 1985, p.692]
Boron
Since 1963, evidence has been accumulating that boron is a safe and effective treatment for some forms of arthritis [Environ Health Perspect. 1994 Nov; 102 Suppl 7: pp.83-5].
- Those with arthritis have been found to have lower boron concentrations in femur heads, bones, and synovial fluid
- Bones of patients using boron supplements are much harder to cut
- In areas of the world where boron intake is usually low (1.0mg or less per day), the incidence of arthritis is 20-70%; in areas where boron intakes are higher (usually 3-10mg), the incidence of arthritis is 0-10%
- Treating osteoarthritis patients with 6mg of boron per day produced positive results in 50% of cases
Dr. Newnham, PhD, DO, ND has demonstrated clear demographic evidence for the usefulness of boron in treating or preventing both rheumatoid arthritis and osteoarthritis. The prevalence of arthritis seems to follow inversely the availability of boron in the soil. [Australian & New Zealand Association for Advancement of Science,1979]
Based on work done at Oxford in the Agriculture Faculty it is believed that at the cellular level mineral metabolism is similar in both plants and man. If this can be relied on, then boron is a membrane catalyst which allows various ions to pass through the cell membrane, particularly phosphates to support synthesis of ATP. This will give energy for efficient repair. It is obvious that in osteoarthritis the cartilage is worn out; if it is because it lacks the necessary energy for cell division, that would explain the action of boron. [Boron and Membrane Function in Plants. Metals and Micronutrients: Uptake and Utilization by Plants. Academic Press; 1983: Ch. 6]
Boron influences calcium and magnesium metabolism, possibly through the parathyroid gland. It does alleviate and seems to cure arthritis either by acting against whatever organism may cause rheumatoid diseases and/or as a membrane catalyst that permits repair of damaged cartilage and collagen.
Copper
The use of copper bracelets in the treatment of arthritis has a long history due to its mild anti-inflammatory effects.
Physical Medicine
Rest
Treatment plans recommended by some doctors include regularly scheduled rest. Others, however, stress the importance of continued mobility during the recovery phase, if tolerated.
Supplements
TMG (Trimethylglycine)
TMG, administered as S-adenosyl-methionine (SAMe), was shown to be superior to ibuprofen (Motrin) in the treatment of osteoarthritis in a double-blind clinical trial. The positive effect in this trial is consistent with several other clinical studies.
Vitamins
Vitamin B5 (Pantothenic Acid)
Low pantothenic acid levels are implicated in the development of human osteoarthritis and rheumatoid arthritis, as whole blood pantothenic acid levels have been reported to be lower in rheumatoid arthritis patients compared with normal controls. In addition, disease activity was inversely correlated with pantothenic acid levels.
Vitamin Niacinamide
Results may be seen in 3-4 weeks with a plateau of improvement reached at 12 weeks. The dose may be lowered at this time but if discontinued, the symptoms will come back. Intake of 500mg 3-6 times daily has commonly been recommended. Sustained release forms require less frequent dosing. [Inflamm Res 1996;45: pp.330-4]
Vitamin E
A clinical trial using 600 IU of vitamin E in patients with osteoarthritis demonstrated significant benefit. The benefit was thought to be due to vitamin E's antioxidant and membrane stabilizing actions. Later studies have shown that vitamin E has an ability to inhibit the enzymatic breakdown of cartilage as well as to stimulate cartilage synthesis.
Report by The Analyst™
Click to see sample report
Click to see sample report
Health problems rarely occur in isolation or for obvious reasons
Your body is a highly complex, interconnected system. Instead of guessing at what might be wrong, let us help you discover what is really going on inside your body based on the many clues it is giving.
Our multiple symptom checker provides in-depth health analysis by The Analyst™ with full explanations, recommendations and (optionally) doctors available for case review and answering your specific questions.
KEY
Weak or unproven link:
may be a sign or symptom of; may suggest; may increase risk of
Strong or generally accepted link:
is often a sign or symptom of; often increases risk of; often suggests
Definite or direct link:
is a sign or symptom of; strongly suggests
Weakly counter-indicative:
may contraindicate; may decrease risk of
May be useful:
may help with
Moderately useful:
often helps with
Very useful:
is highly recommended for
Last updated: Jan 01, 2023